
使用脉冲颅扩张波形的无创颅内压估计的机器学习方法
作者:Hu, Xiao
在过去的两个世纪中,研究表明,在颅内室之间保持平衡对于大脑功能至关重要,因为颅内压(ICP)降低了脑血液灌注并破坏大脑血流的调节
1。颅内体积和压力之间的关系,是颅内依从性的代理(ICC)2,是颅内动力学状态的重要指标。
除了监测脑组织氧合,代谢和电活动之类的因素外,评估ICC在神经行为护理领域中至关重要3。然而,ICP监测的黄金标准以及先前提出的ICC监测系统涉及将侵入性探针放入心室或脑实质中4,,,,5。侵入性方法虽然有效,但受到专业人员执行程序,实质性成本以及与侵入性大脑程序相关的固有风险的限制。
为了解决ICP升高的更广泛背景,必须认识到导致这种情况的各种根本原因,包括脑外伤(TBI),颅内出血,脑积水,肿瘤,肿瘤和严重的缺血性中风。这些条件破坏了颅内室之间的微妙平衡,导致ICP和相关并发症增加,例如脑灌注减少和潜在的疝。确定可以从非侵入性ICP测量中受益的人群同样至关重要。高危人群,例如神经严重护理部门的患者,患有慢性神经系统疾病的人或需要立即进行ICP评估的患者,例如在战场或紧急情况下,将从更安全的无创替代方案中大大受益。非侵入性方法的主要优点在于它们的潜力减少程序风险,增强对资源有限的设置中ICP监视的可访问性,并提供动态的实时评估。
为了追求更安全的医疗实践,现代的无创技术已经出现,为医师提供了在各种临床情况下调查颅内高血压(IH)的宝贵工具。这些技术包括经颅多普勒(TCD),视神经鞘直径(ONSD)超声检查,读式计量。ICP6。
提出了TCD作为一种通过计算方法监测ICC的方法,该方法考虑了大脑动脉床和脑脊髓空间的隔室合规。但是,直接的ICP监视无法用这种方法代替7。最近,另一种无创方法加入了研究ICC和IH脑4CARE(B4C)系统的一系列工具8。这个新型的机械传感器可以检测微米脉冲颅膨胀起源于每个心脏周期内的ICP变化。B4C系统已经证明了捕获替代ICP脉冲形态(ICP波形ICPW)的能力,这是一种与ICC紧密相关的生理体征9。B4C系统的高灵敏度允许其检测幅度为0.04至0.80 mm的脑脉动10,这导致相应的微米脉冲颅膨胀。该系统还提供自动波形分析,并将ICP变化转化为数字参数(例如P2/P1比,p2/p1的比率,时间到峰[TTP])在床边实时,从而增强了患者的动态监测。11,,,,12。P2波(潮汐)遵循ICP波形中的P1波(打击乐波)。升高的P2/P1比表明ICC降低,表明大脑补偿颅内体积增加的能力降低。此外,TTP(从ICP波开始到其最高峰的持续时间)提供了有关颅内系统响应的信息:较短的间隔表示高ICC,而较长的间隔表示较低,有害的ICC13。
人工智能(AI)的进步,尤其是机器学习领域(ML),无论是用于聚集动脉血压(ABP)还是TCD波形以估算ICP的大脑监测潜力很大14和ICPW15评估,甚至用于确定ICP监测的并发症,例如心室炎16。
尽管有这些有希望的发展,但无创床旁ICP估计仍然难以捉摸。因此,本研究的主要目的是利用B4C系统获得的ICPW记录的大量数据集,并采用ML技术来在神经智力护理环境中同时进行ICP监测的患者中无创地估算ICP值。其次,将该模型与基于TCD的先前报道的无创方法进行了比较,以提供临床性能的基线评估。
结果
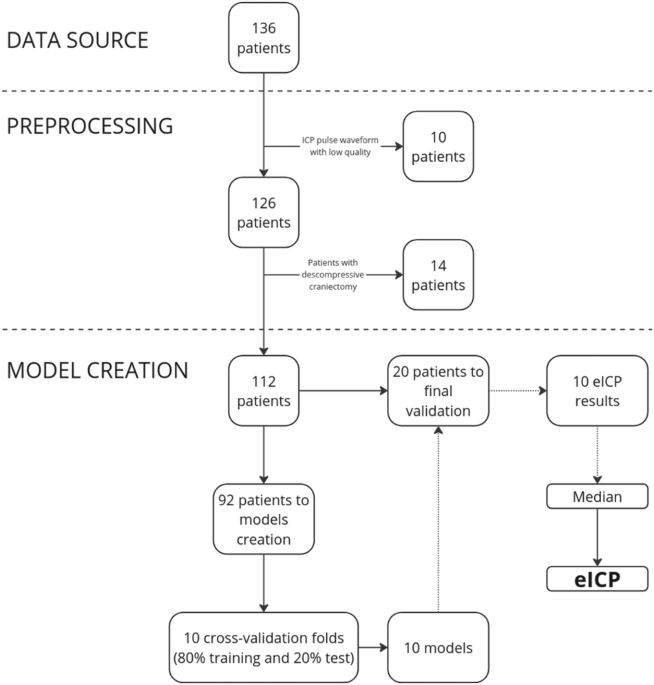
总共考虑了136名患者进行评估。由于合并的非侵入性ICPW(NICPW)形态质量低,因此将10名患者排除在初始组中,例如运动伪像的存在和不可靠的波形)或不可靠的监测持续时间,从而导致了126名患者的修订池。随后,另外14例进行了减压颅骨切除术的患者被切除,导致112名患者的数据被分割成10 s窗户,总共有11,604个窗户,相当于15万脉冲(图。1)。桌子1代表模型开发和模型验证的人口样本人口统计和数据分配。
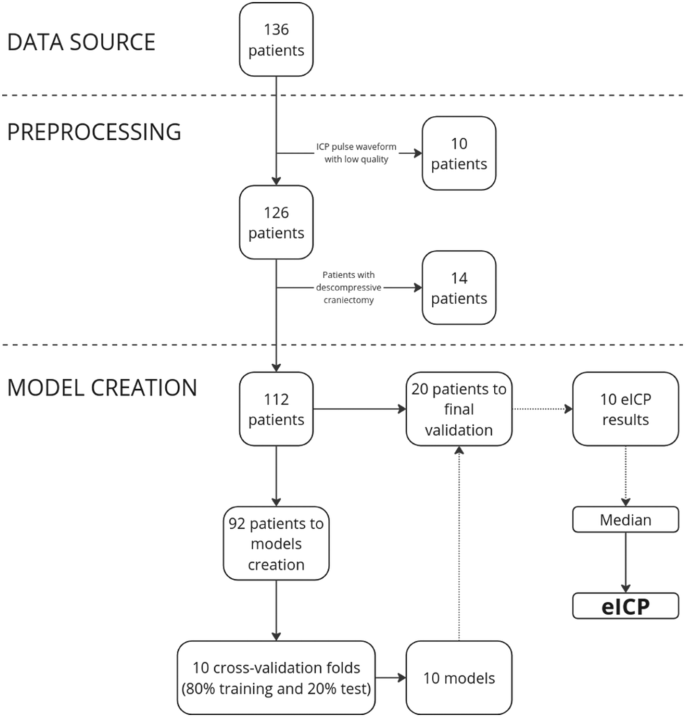
该图提供了数据源,患者选择程序和模型培训工作流程的概述。
总体而言,整个人口样本(n= 112)显示了5.36%的数据,值高于20 mmhg(表1)。在模型开发样本中,有86.6%的患者患有外心室排水(EVD),而14.4%的患者患有ICP内部ICP换能器,而在验证样本中,100%的患者具有EVD。
Windows <20 mmhg的ICP为11.89±3.21(n= 1996年)和21.26±1.67 windows> 20 mmhg(n= 17)在验证样本中。负预测值(NPV)为0.99,正预测值(PPV)为0.14。模型的交叉验证折叠显示的平均绝对误差(MAE)为1.23±0.02 mmHg,平均平方误差(MSE)为3.68±–
测试数据集的0.34 mmHg。对于火车数据集,MAE为0.91±0.01 mmHg,MSE为1.88±0.05 mmHg。桌子2显示了10个折叠中每一个的模型交叉验证误差分布。验证数据集的MAE为3.00 mmhg,MSE为13.56 mmhg(n= 20,2013 10-S Windows)。这些值与实际ICP的变化是同步的,例如,如图2所示。2。图2:侵入性和非侵入性颅内压(ICP)方法的并发趋势。该图显示了2013年的概述,该概述是从验证数据集获得的并发平均侵入性ICP(蓝色)和无创估计的ICP(EICP)(RED)值(RED)值(RED)值(RED)(RED)值(

= 20)。可以在补充图2中观察到每个患者的个体趋势。13。表2对于模型的交叉验证折叠(MMHG中的值)的平均绝对误差(MAE)和平方误差(MSE)
3显示验证数据集的无创估计的ICP(EICP)值,该值显示了ICP和EICP的平均值,以及每个患者观察到的差异。补充图2中介绍了每个验证患者的ICP和EICP时间趋势的图形分析。13。
平淡的Altman分析表明,ICP和EICP之间的平均差异(偏差)为0.21 mmHg,SD为±3.68 mmHg。从这些值中,ICP预测少于±7.5 mmHg的置信度限制为95%(图。3)。ICP和EICP之间存在适度的关系(r= 0.43,p<0.05),如图2所示。4。图3:侵入性和非侵入性颅内压(ICP)方法之间的一致性。该图代表了比较实际的ICP与非侵入性估计的ICP(EICP)的平淡图。

实际ICP与无创估计的ICP(EICP)之间关系的散点图。

代表长矛人相关系数。当计算每个10 s窗口的EICP均值时,在36.61%的验证窗口中获得了低于2 mmHg的实际ICP的差异,如图2所示。5。
对于10张窗口的71.90%,差异低于4 mmHg,而对于91.48%的窗口,错误低于6 mmHg。重要的是要注意,<9%的窗户在ICP和EICP> 6击之间显示出差异,如图2所示。5。此外,对具有ICP <20 mmHg和ICP的20 mmhg的10窗口之间的平均差异进行了分析。据观察,对于第一组而言,MAE为2.97 mmhg,而对于第二组来说,MAE为6.41 mmhg。由于ICP升高范围内的数据点数量有限,因此预期观察到的结果。尽管努力平衡培训和测试数据集,但5.36%的数据点高于20 mmHg,限制了IH有效的模型培训。

该图显示了每个10 s窗口的ICP和EICP值之间的差异,表明<9%的窗口显示错误> 6 mmHg。ICP颅内压,EICP估计的颅内压。
EICP和EICP的比较TCD
桌子4显示EICP和EICPTCD验证数据集患者的个人值(同时进行B4C和TCD测量)(n= 13),显示ICP,EICP和EICP的平均值TCD,以及每个患者观察到的差异。表4 EICP(基于Brain4Care)和EICP之间的性能比较
TCD。ICP预测的95%置信区间(95%CI)为EICP的±4.17 mmHg,EICP的±10.78 mmHgTCD。ICP和EICP之间有很强的关系(Spearmanr= 0.76,p<0.05),ICP和EICP之间没有显着关系TCD(斯皮尔曼r= 0.25,p= 0.40)。讨论
提出的ML模型使用来自大型临床数据库的众多NICPW功能,估计2013年急性脑损伤(ABI)患者的平均ICP在2013年的MAE中为3.00 mmhg,在ICP预测下为95%CI,低于ICP的CI。
±7.5 mmhg。这些发现推动了ICP的研究和临床使用,并有望在神经严峻的患者之外使用可靠的非侵入性ICP方法。
当前管理神经严格患者的标准正在接受审查,尤其是在定义可靠的阈值时,该阈值表明何时ICP和脑灌注压力(CPP)值需要升级的干预措施17。该领域的学者强烈建议一种积极的方法,强调了预期IH事件以增强患者预后的重要性18,,,,19。在这种情况下,ICPW的作用变得关键,因为这些波形的变化可以作为即将发生IH潮流的早期指标,并且是ICC损害的可靠标记13。此外,ICPW已被证明可以有效预测患者的预后20,,,,21。通过使用实用B4C系统的EICP开发,该系统已经处理了ICPW参数(例如P2/P1比率和TTP),其目的是在预测IH事件方面取得了重大飞跃。这种开发提供了EICP形式的宝贵指南,以及通过NICPW参数对预测进行微调,从而提供了一种全面的方法来管理ICP并有可能改善患者的结果。
迄今为止,已经探讨了估计人类无创ICP值的各种方法。这些方法采用了TCD和ABP波形等技术15,,,,22,,,,23,,,,24,,,,25,声学信号26,,,,27,或ONSD超声检查28,所有这些都显示出令人鼓舞的结果。但是,文献表明用于确定这些非侵入性ICP估计方法的准确性的指标有显着差异,通常以平均绝对差异(MAD),MAE和95%CI测量。在这项研究中,MAE和MSE都被用作评估指标,以提供对模型性能的互补见解。MAE被选为与临床实践的一致性,其中平均与真实值的平均偏差更直观地理解并与每日ICP评估一致。包括MSE强调较大的偏差,这对于ICP测量特别重要,因为它们的潜在临床意义。此外,使用MAE与监管标准相一致,例如医疗仪器促进协会(AAMI,NS28:1988(R2015))和脑创伤基金会(BTF)指南29,指定ICP监视的准确性要求。
在一项开创性研究中,Schmidt等人。24提出了利用ABP和TCD脑血液速度来计算非侵入性ICP的线性模型,报告了4.0±1.8 mmHg的MAD。通常,基于TCD的模型类别中的非侵入性ICP方法显示出不同的精度,95%CI范围从大约±10±10′20 mmHg不等6,,,,14,,,,25,,,,30。最佳基于光学ONSD的ICP估计的研究最多呈现95%CI为±7.58 mmHg28。
对本研究中提出的模型(EICP)的比较分析TCD,一种基于TCD的CPP的文献中建立的良好方法30,,,,31,,,,32,突出显示其性能的显着差异。尽管EICP与ICP表现出更紧密的一致性和更强的相关性,但EICPTCD表现出较少的精度(95%CI为±10.78 mmHg),与ICP无显着关系。这种比较分析在患者的一部分中为评估提供了基线,并强调了该模型的潜在优势,这是一种更准确和可靠的无创方法。但是,有必要进行更广泛的验证,包括在不同的临床条件和其他非侵入性ICP估计方法之间进行的前瞻性比较。
最近的研究探索了其他创新模型,用于无创ICP估计。例如,Jaishankar等人。22开发了将ABP和脑速度波形相关的频域模型。他们的研究涉及五名患者的数据,得出的平均误差为1.5 mmHg,误差的标准偏差为4.3 mmHg22。同样,Megjhani等人。15构建了一个ML框架,其中包含来自ABP,心电图(ECG)和TCD波形的数据。他们的发现表明,基于13位患者的数据,针对域的对抗神经网络模型的MAE为3.88 mmHg,域对抗变压器模型的MAE和3.94毫米的MAE MAE和3.94毫米。15。作者还表示在±10 mmhg范围内有95%CI15。
在另一种方法中,Ganslandt等人。26采用声学信号发射技术,观察到95%CI为±7.92 mmHg,在2543个数据点中有85%的差异为5 mmHg(n= 14名患者)。最近,一项使用长距离NIRS数据的研究报告说,随机森林模型的最低MAE为5.030 mmHg,宽95%CI范围从8.782到8.487 mmHg33。总的来说,这些研究突出了估计ICP的准确性以及精度指标定义以比较侵入性和无创ICP的定义的巨大变化。
虽然临床指南通常建议特定的阈值值,例如将ICP水平保持在22毫米低于60 mmHg以上的ICP水平以触发治疗升级34,越来越认识到ICP管理应该更加个性化,并且有细微的差别35。这强调了非侵入性ICP估计作为提供个性化和动态的ICP管理的有价值工具的潜在实用性,尤其是具有能够高精度的模型。
实际上,ICP测量的准确性在临床实践中至关重要。根据AAMI(NS28:1988(R2015))和BTF指南的标准29,ICP监视设备应在0 100 mmHg范围内连续输出,其准确性为0αmmHg范围,ICP的最大预测误差为10%。> 20 mmhg。值得注意的是,先前提出的非侵入性ICP数据驱动模型虽然有价值,但可以表现出不同程度的平均误差,范围从±5到20 mmHg,通常伴随着高标准偏差6。
在神经关怀中,实时ICP估计的一种无创方法对于主动的患者管理和早期干预至关重要,最终导致结果改善。尽管ICP的标准参考值通常范围为5至15 mmhg,但文献中有关升级或降低疗法强度的确切阈值的文献存在持续的辩论17,,,,36,,,,37。最近的一项研究探讨了ABI患者中ICP值与B4C测得的P2/P1比率之间的协同关系11。这项研究表明,ICC的非侵入性标志物可以区分短期结局,这表明与P2/P1比率正常的患者相比,P2/P1比率升高的患者的结局较差,即使ICP值相似(15)(15â(15))25 mmhg)。
因此,可以通过在整个临床过程中连续监测患者的颅内动力学来得出动态和个性化的ICP基线。正如Godoy等人强调的那样,这与对颅内生理的不断发展的理解相吻合。38,将ICC及其障碍优先考虑在ICP波形形态的变化上,而不是刚性ICP阈值。例如,诸如P2/P1比率之类的波形特征是ICC损伤的敏感标志物,从而提供了与患者特定基线的偏差的见解。
在这项研究中开发的ML模型利用了脑4CARE技术,通过基于波形形态提供无创的实时ICP估计来促进这种个性化的方法。曲线下的P2/P1比,TTP和区域之类的功能使ICC损害的早期检测,诸如Neurovanguard方法等策略等策略39,它整合了侵入性和无创方法,以进行更准确的评估。此外,辅助技术,例如TCD,近红外光谱(NIRS)和ONSD超声可以有助于基线测定,从而提供有关大脑依从性,氧合和血液动力学的多模式观点。
通过将这些高级工具与护理标准措施(包括神经影像学和神经学评估)相结合,临床医生可以为每个患者构建一个全面而动态的基线。这种个性化的方法允许早期识别关键趋势,实现及时的干预措施,并在可行的情况下降低对侵入性程序的依赖。这些策略强调了实时,非侵入性ICP监测的价值以及ML在优化颅内动力学管理方面的整合,最终改善了神经政治的护理结果。
B4C系统的优势取决于处理的简单性,即时信息获取,缺乏任何类型的能量排放以及对较低财务资源位置的适用性,就像使用一种设备一样,可以密切监控几名患者12。此外,B4C系统的NICPW在Beat-Beat基础上代表了ICP动力学的真实生理信号,这与非侵入性ICP估计的其他模型相比,这是一个优势,该模型仅利用与ICP动力学相关的二级参数,例如基于TCD的大脑血液速度和平均ABP。在这种情况下,提出的模型更有优势,因为它依赖于单个生理信号,避免了由多参数架构引起的潜在差异。此外,对于近40%的验证样本,所提出的模型能够在AAMI建议的误差范围内执行(±2 mmHg)。
依靠替代ICP脉冲形态的拟议方法简化了数据获取并提供了更好的准确性。尽管需要进一步的完善,尤其是对于模型的性能尚不足以独立临床决策的边缘案例,这项研究为临床可行,无创的ICP监测工具奠定了基础模型优化。
尽管与EICP相比表现出卓越的性能TCD鉴于该领域的先前报告,提出的ML模型需要在较大的患者人群中进行进一步的前瞻性验证,以评估其在不同临床环境中的普遍性和鲁棒性。这还将允许收集更广泛的ICP值,这在本研究中受到限制。此外,提出的模型显示了基于训练样品组成的方差,并且尚不可推广到ABI以外的临床状况。
诸如颅骨切除术等手术的颅骨缺陷较大的患者会表现出改变的颅内动力学,可能会影响B4C系统的准确性40。但是,ICP脉冲形态在这些患者中的价值表明,B4C系统仍可能提供有价值的见解41。一个值得注意的限制是对患者躁动的敏感性,这可以降低信噪比(SNR)和阻碍波形读数。最大程度地减少患者躁动的影响对于优化系统的性能至关重要。建议进行监督的监视以确保可靠的数据收集。另一个局限性涉及如果传感器在主要的颅外动脉附近置于颅外循环脉冲造成信号污染的风险。正确的传感器定位可以消除这些文物。B4C系统包括控制措施,例如识别和警告的应用程序算法,该算法警告了由不当放置或过度伪像引起的信号不足,从而确保了适当的数据收集以进行临床解释。
这项研究的一个潜在局限性是利用核内层层腔内和脑室内ICP传感器,这可能引入测量误差。系统的综述和荟萃分析发现,不同侵入性ICP监测方法之间的这些错误约为1.5毫米(95%CI 0.7 2.3)42。尽管通常可以忽略不计,但这种可变性可能会影响提出的模型的准确性,从而强调了其仔细验证的需求。
与以前的报道相比,用于生成ML模型的大种群样本量是本研究的强度。但是,即使在15英寸的20 mmHg范围内,数据集中ICP值的低多样性也可能导致对实际ICP的EICP高估(图。4),这可能导致不必要的治疗。这表明当前的方法需要改进。未来的努力将重点放在数据增强和培训模型上,并具有更大的临床多样性数据集,IH事件分布更高。在此阶段,在评估平均压力值时,模型精度较高。在寻求临床调节清除之前,该模型的未来迭代将使用较大的数据集进行完善,以增强估计动态并减少低估和高估之间的时间波动。
总而言之,本研究证明了使用专门从非侵袭性获得的脉冲颅扩张波形估算ICP的潜力。虽然需要进一步的前瞻性验证来确认该ML模型的临床实用性,但无创的ICP估计的开发显示出了希望。这种进步可能使ICP成为更广泛的生命体征,从而有可能改善各种临床环境中的识别,治疗选择和预测过程。
方法
研究设计和人口
这是对在巴西四个中心独立进行的前瞻性观察研究的回顾性分析,包括圣保罗大学医院DAS诊所(IRB,参考号6150621,CAAE:39348920.1.1.1001.0068),Sao of Sao University of Sao University of Sao University of Sao University of Sao University of Sao大学Paulo (IRB reference number 3.129.120, CAAE: 03843118.0.0000.5505), Hospital João XXIII (IRB under the reference number 6150621, CAAE: 39348920.1.1001.0068) and Hospital Estadual de Emergência e Trauma Senador Humberto Lucena (IRB reference number 5.078.425,CAAE:39348920.1.2001.5186);波尔图大学的Sao Joao医院(IRB参考编号106-17)的葡萄牙一个中心;以及美国的两个中心,斯坦福大学(IRB参考编号46100)和约翰·霍普金斯大学(IRB参考号IRB00204065)。研究方案是根据赫尔辛基宣布的,并获得了每个各自中心的当地伦理委员会的批准,并获得了患者或其合法授权代表的知情同意。根据增强流行病学(Strobe)标准的观察性研究的报告(https://www.strobe-statement.org/checklists/)。
2015年1月1日至2024年1月1日,在各个中心入院的患者,如果他们经历了在入院后的前五天内经历了需要侵入性ICP监测的ABI,则有资格纳入本研究。该研究排除了进行了减压颅骨切除术或表现出脑死亡迹象的患者。对于涉及TBI的案件,BTF指南制定的高脑部催眠风险指南29紧随其后。在蛛网膜下腔出血的情况下,管理程序相似,尽管重要的是要注意,目前缺乏非创伤ABI病例中ICP管理的具体准则43。值得一提的是,患者护理是独立于本研究进行的,并且使用B4C传感器获得的数据并未用于临床决策或患者管理。
神经监测
根据临床适应症,通过光纤纤维内充质换能器(Raumedic,Munchberg,德国)监测ICP。B4C系统(Brain4Care,Sao Carlos,Sao Paulo,Brazil)是由食品药物管理局清除的可穿戴传感器(FDA数字K201989),用于注册NICPW。先前的研究详细描述了其操作原理8。总而言之,B4C系统涉及将高度敏感的传感器与皮肤接触到颅骨上,该传感器检测到源自ICP变化的每个心脏周期的微米脉冲颅膨胀。在多个临床研究中,使用B4C系统获得的波形的形态特征已被始终证明与侵入性ICP相关11,,,,12,,,,40,,,,44,,,,45。
将B4C系统放置在与ICP探针植入同一侧的额叶区域。从不同患者样品中取出的同时记录是由侵入性ABP,ICP和非侵袭性脉冲颅扩张波形(B4C系统)制成的。For the data collected at the Sao Paulo University’s Hospital das Clinicas, additional recordings of ECG, temperature, oxygen saturation, and middle cerebral artery (MCA) blood velocity with TCD were taken.The primary purpose of establishing this database was to investigate variations in ICP in relation to MCA blood velocities and cerebrovascular autoregulation46,,,,47, as well as invasive and noninvasive ICP waveforms40。
The collected data consisted of several short recording sessions, each lasting at least 10 min, and electronically acquired and synchronized from patient bedside monitors at a sampling frequency of 250 Hz using an in-house data collection system (brain4care, Sao Carlos, Sao Paulo, Brazil). During these sessions, strict monitoring by the investigator in charge was maintained to prevent any displacement of the B4C sensor, which could potentially compromise the quality of the signal. Investigators participating in the data collection were not part of the direct care team. Also, the direct care team did not have access to the data during collection.
信号处理
Initially, the power spectral density derived from the B4C signal was used to estimate the SNR, calculated as the ratio of signal energy within the fundamental frequency and its first three harmonic frequencies, compared to the spectral range spanning from 0.1 to 25 Hz. Signals exceeding an SNR threshold of 0.35 underwent mean pulse assessment serving as the input for a quality classifier to determine signal morphology acceptability. The output of this classifier indicated whether a signal met quality standards, having passed these two assessment stages. For downsampled signals, standardizing sample rates ensured uniformity across all signals. The data curation process was rigorous, with initial data parsing, detrending, signal validation, filtering, inversion verification, pulse identification, artifact removal, pulse alignment, pulse averaging, and pulse parameter calculation performed by analytical software in the B4C System cloud. Signal filtering involved a two-part algorithm: a 0–1 signal quality index based on spectral analysis of one-minute downsampled and detrended data, followed by a binary classifier trained on 21,000 manually classified pulses.
For the invasive ICP signal, no signal processing was applied to derive the averaged ICP values.
Proposed machine learning framework
The model utilized for estimating ICP employed a histogram gradient boosting (HGB) regressor48, an ensemble learning technique that sequentially trains decision trees to correct errors made by previous trees. This approach effectively captures complex relationships and non-linear patterns in the data by constructing trees based on histograms of feature values. HGB was the model of choice based on a comparative analysis with other models such as temporal convolutional network (TCN) and convolutional neural network (CNN), as it provided the best estimation accuracy and requires less computational power. A quantitative comparison of the performance of each model tested is presented in Supplementary Table1。
The feature engineering process involved extracting various parameters from the B4C waveform. This process resulted in the extraction of approximately 1110 features, described in Supplementary Note1。These features were then refined based on their Spearman correlation coefficient with the regression target—the invasively obtained ICP values in these patients, and subsequently with their calculated importance.Feature importance was determined by prioritizing features with higher correlation coefficients.Redundant features were excluded in favor of the next most important feature, resulting in 15 features.The correlation coefficients between each feature and ICP are also described in Supplementary Note1。The detection of redundant features was based on two types of correlation.First, the correlation between features is assessed.If two features are highly correlated, it indicates they provide similar information, which can lead to redundancy.Redundant features are excluded in favor of the next most important feature, ensuring that only unique and valuable information is retained.This step helps eliminate unnecessary complexity without sacrificing predictive power.Second, the correlation between each feature and the target variable is evaluated.Features that show little to no correlation with the target are unlikely to contribute meaningfully to the model’s predictions and are subsequently excluded.
To optimize model performance, hyperparameters underwent selection through a grid search approach with a primary focus on achieving the optimal MAE and MSE for the training dataset while avoiding undersampling or oversampling through cross-validation with 10 folds and analysis of hyperparameters.桌子5describes the key elements for processing and optimization of the proposed model.补充表2summarizes results obtained for each combination of hyperparameters to arrive at the final model selection.
To address the imbalances in the dataset, e.g., the limited representation of IH data (ICP > 20 mmHg), a class weighting scheme that assigns weights inversely proportional to the frequency of each class was implemented for the model development phase. This method ensures that cases with lower representativity, e.g., IH events, are given greater importance during the training process, thereby improving the model’s performance on these critical cases. By calculating the frequency of normal and elevated ICP instances and mapping these frequencies to their corresponding weights, the model’s ability to learn from the imbalanced data can be enhanced, ultimately leading to more accurate predictions across all ICP ranges.
Parameters derived from B4C nICPW morphological segments (e.g., P2/P1 ratio, TTP, area under the curve, intracranial compliance scale49) and outcomes of dimensionality reduction techniques were utilized in the development of this proprietary (patent-pending) predictive model. The Isomap dimensionality reduction technique was applied to the raw waveform signals, resulting in 25 reduced-dimensional fragments (Supplementary Note1) used as input features for the model. To ensure model simplicity and avoid redundancy, the inclusion of these fragments was carefully analyzed alongside the raw features. Features were refined based on their correlation with the regression target (ICP) and their importance to the model as described above. Importantly, no parameters derived from any other physiological signals were included in the model.
The entire workflow embraced a robust 10-fold cross-validation strategy to ensure the reliability of the model. This strategy involved separating data from the same patient between training and testing in each fold, with 80% allocated for model training and 20% for testing. Additionally, data from 20 patients were set aside for final replication and validation, with their data held separate and not utilized in the model development phase.
After model training, saved models from each fold were used to estimate ICP values in the validation dataset (n = 20). The model produced 10 calibrations and the resulting estimated ICP value (eICP) was determined as the median of these calibration models.Python 3.7, in a Jupyter Notebook environment hosted on a high-performance server, was utilized for model development due to its flexibility and extensive libraries for ML tasks.
Comparison with a baseline noninvasive method
Czosnyka et al.
50proposed a method based on diastolic cerebral blood velocity for the estimation of noninvasive cerebral perfusion pressure (nCPP). Studies in the literature have demonstrated that such patterns of the TCD waveform reflect impaired cerebral perfusion caused by a decrease in CPP50,,,,51。With this method, ICP can be estimated as the difference between ABP and nCPP (eICPTCD = ABP−nCPP)30,,,,31,,,,32。nCPP estimation is expressed as (Eq. (1)):$${\rm{nCPP}}={\rm{ABP}}\times \frac{{\rm{F}}{{\rm{V}}}_{{\rm{d}}}}{{\rm{F}}{{\rm{V}}}_{{\rm{m}}}}+14\,{\rm{mmHg}}$$
(1)
FV
dand FVm(cm/s) represent diastolic and mean blood velocity from the MCA, respectively. 14 mmHg is a preestablished calibration (zeroing) parameter derived from TBI patients.To provide a comparative baseline assessment with an established method previously reported in the literature, the proposed eICP model was compared with eICP
TCDin a subset of cases from the validation dataset with patients who had concurrent B4C and TCD measurements (n = 13).统计分析
The model was statistically assessed through the utilization of MAE, MSE, Bland–Altman plot for comparison of ICP with eICP, 95% CI for ICP prediction, and the Spearman correlation between ICP and eICP values.
The Shapiro–Wilk test was used to test the normality of the distribution of the variables.Mean ± standard deviation (SD) was utilized to evaluate the outcomes of the patient sample.一个pvalue < 0.05 was considered for statistical significance. The statistical calculations were also carried out using Python 3.7.For this observational study, the sample size was determined based on the availability of participants meeting inclusion criteria and practical constraints such as time and resources. While acknowledging the convenience-based nature of the sample, efforts were made to ensure representativeness within these limitations.
数据可用性
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
代码可用性
The underlying code for this study [and training/validation datasets] is not publicly available for proprietary reasons.
参考
Smith, M. Cerebral perfusion pressure.
br。J. Anaesth。 115, 488–490 (2015).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Lanier, W. L. & Warner, D. O. Intracranial elastance versus intracranial compliance: terminology should agree with that of other disciplines.麻醉学 77, 403–404 (1992).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Citerio, G. et al. International prospective observational study on intracranial pressure in intensive care (ICU): the SYNAPSE-ICU study protocol.BMJ开放 9, e026552 (2019).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Piper, I. R., Miller, J. D., Whittle, I. R. & Lawson, A. Automated time-averaged analysis of craniospinal compliance (short pulse response).Acta Neurochir.补充。 51, 387–390 (1990).
CAS一个 PubMed一个 Google Scholar一个
Yau, Y. H., Piper, I. R., Clutton, R. E. & Whittle, I. R. Experimental evaluation of the Spiegelberg intracranial pressure and intracranial compliance monitor. Technical note.J. Neurosurg。 93, 1072–1077 (2000).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Zhang,X。等。Invasive and noninvasive means of measuring intracranial pressure: a review.生理学。测量 38, R143–r182 (2017).
文章一个 PubMed一个 Google Scholar一个
Kim, D. J. et al. The monitoring of relative changes in compartmental compliances of brain.生理学。测量 30, 647–659 (2009).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Andrade, R. d. A. P. A nanometer resolution wearable wireless medical device for non invasive intracranial pressure monitoring.IEEE Sens. J. 21, 22270–22284 (2021).
文章一个 CAS一个 Google Scholar一个
Kazimierska, A. et al. Analysis of intracranial pressure pulse waveform in studies on cerebrospinal compliance: a narrative review.生理学。测量 44,,,,https://doi.org/10.1088/1361-6579/ad0020(2023)。
Almudayni, A. et al. Magnetic resonance imaging of the pulsing brain: a systematic review.岩浆 36, 3–14 (2023).
文章一个 PubMed一个 Google Scholar一个
Brasil, S. et al. Noninvasive intracranial pressure waveforms for estimation of intracranial hypertension and outcome prediction in acute brain-injured patients.J. Clin。监视。计算。 37, 753–760 (2023).
文章一个 PubMed一个 Google Scholar一个
Brasil, S., Godoy, D. A. & Hawryluk, G. W. J. A point-of-care noninvasive technique for surrogate ICP waveforms application in neurocritical care.Neurocrit.关心 https://doi.org/10.1007/s12028-023-01786-2(2023)。
Brasil, S. et al. A comprehensive perspective on intracranial pressure monitoring and individualized management in neurocritical care: results of a survey with global experts.Neurocrit.关心 https://doi.org/10.1007/s12028-024-02008-z(2024)。
Kashif, F. M., Verghese, G. C., Novak, V., Czosnyka, M. & Heldt, T. Model-based noninvasive estimation of intracranial pressure from cerebral blood flow velocity and arterial pressure.科学。翻译。医学 4, 129ra144 (2012).
文章一个 Google Scholar一个
Megjhani, M. et al. A deep learning framework for deriving noninvasive intracranial pressure waveforms from transcranial Doppler.安。神经。 94, 196–202 (2023).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Megjhani, M. et al. Dynamic intracranial pressure waveform morphology predicts ventriculitis.Neurocrit.关心 36, 404–411 (2022).
文章一个 PubMed一个 Google Scholar一个
Wijdicks, E. F. M. 10 or 15 or 20 or 40 mmHg? What is increased intracranial pressure and who said so?Neurocrit.关心 36, 1022–1026 (2022).
文章一个 PubMed一个 Google Scholar一个
Bradley, G. R. E., Roldán, M. & Kyriacou, P. A. Machine learning approaches to intracranial pressure prediction in patients with traumatic brain injury: a systematic review.应用。科学。 13, 8015 (2023).
文章一个 CAS一个 Google Scholar一个
Güiza, F., Depreitere, B., Piper, I., Van den Berghe, G. & Meyfroidt, G. Novel methods to predict increased intracranial pressure during intensive care and long-term neurologic outcome after traumatic brain injury: development and validation in a multicenter dataset.暴击。护理医学。 41, 554–564 (2013).
文章一个 PubMed一个 Google Scholar一个
March, K. Intracranial pressure monitoring and assessing intracranial compliance in brain injury.暴击。Care Nurs.临床北部。 12, 429–436 (2000).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Mataczynski, C., Kazimierska, A., Uryga, A. & Kasprowicz, M. Intracranial pressure pulse morphology-based definition of life-threatening intracranial hypertension episodes.安努。int。conf。IEEE Eng.医学生物。Soc。 2022, 1742–1746 (2022).
PubMed一个 Google Scholar一个
Jaishankar, R. et al. A frequency-domain approach to noninvasive intracranial pressure estimation.安努。int。conf。IEEE Eng.Med Biol。Soc。 2019, 5055–5058 (2019).
PubMed一个 Google Scholar一个
Imaduddin, S. M., Fanelli, A., Vonberg, F., Tasker, R. C. & Heldt, T. Pseudo-Bayesian model-based noninvasive intracranial pressure estimation and tracking.IEEE Trans。生物。工程。 https://doi.org/10.1109/TBME.2019.2940929(2019)。
Schmidt, B., Klingelhöfer, J., Schwarze, J. J., Sander, D. & Wittich, I. Noninvasive prediction of intracranial pressure curves using transcranial Doppler ultrasonography and blood pressure curves.中风 28, 2465–2472 (1997).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Cardim, D. et al. Non-invasive monitoring of intracranial pressure using transcranial Doppler ultrasonography: is it possible?Neurocrit.关心 25, 473–491 (2016).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Ganslandt, O., Mourtzoukos, S., Stadlbauer, A., Sommer, B. & Rammensee, R. Evaluation of a novel noninvasive ICP monitoring device in patients undergoing invasive ICP monitoring: preliminary results.J. Neurosurg。 128, 1653–1660 (2018).
文章一个 PubMed一个 Google Scholar一个
Herklots, M. W. et al. Prospective evaluation of noninvasive headsense intracranial pressure monitor in traumatic brain injury patients undergoing invasive intracranial pressure monitoring.世界神经外科。 106, 557–562 (2017).
文章一个 PubMed一个 Google Scholar一个
Robba, C. et al. Optic nerve sheath diameter ultrasonography at admission as a predictor of intracranial hypertension in traumatic brain injured patients: a prospective observational study.J. Neurosurg。 132, 1279–1285 (2019).
文章一个 PubMed一个 Google Scholar一个
Carney, N. et al. Guidelines for the management of severe traumatic brain injury, Fourth Edition.神经外科 80, 6–15 (2017).
文章一个 PubMed一个 Google Scholar一个
Rasulo, F. A. et al. Transcranial Doppler as a screening test to exclude intracranial hypertension in brain-injured patients: the IMPRESSIT-2 prospective multicenter international study.暴击。关心 26, 110 (2022).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Rasulo, F. A. et al. The accuracy of transcranial Doppler in excluding intracranial hypertension following acute brain injury: a multicenter prospective pilot study.暴击。关心 21, 44 (2017).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Cardim, D. et al. Prospective study on noninvasive assessment of intracranial pressure in traumatic brain-injured patients: comparison of four methods.J. Neurotrauma 33, 792–802 (2016).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Bradley, G. R. E. & Kyriacou, P. A. Evaluating the effectiveness of non-invasive intracranial pressure monitoring via near-infrared photoplethysmography using classical machine learning methods.生物。信号过程。控制 96, 106517 (2024).
文章一个 Google Scholar一个
Hawryluk, G. W. J. et al. A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC).重症监护医学。 https://doi.org/10.1007/s00134-019-05805-9(2019)。
Smith, M. & Maas, A. I. R. An algorithm for patients with intracranial pressure monitoring: filling the gap between evidence and practice.重症监护医学。 45, 1819–1821 (2019).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Kofke, W. A. et al. Defining a taxonomy of intracranial hypertension: is ICP more than just a number?J. Neurosurg。Anesthesiol. 32, 120–131 (2020).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Riparbelli, A. C. et al. Critical ICP thresholds in relation to outcome: Is 22 mmHg really the answer?Acta Neurochir.166, 63 (2024).
文章一个 PubMed一个 Google Scholar一个
Godoy, D. A., Brasil, S., Iaccarino, C., Paiva, W. & Rubiano, A. M. The intracranial compartmental syndrome: a proposed model for acute brain injury monitoring and management.暴击。关心 27, 137 (2023).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Rodriguez, E. E., Zaccarelli, M., Sterchele, E. D. & Taccone, F. S. “NeuroVanguardâ€: a contemporary strategy in neuromonitoring for severe adult brain injury patients.暴击。关心 28, 104 (2024).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Brasil, S. et al. A novel noninvasive technique for intracranial pressure waveform monitoring in critical care.J. Pers。医学 11,,,,https://doi.org/10.3390/jpm11121302(2021)。
Brasil, S. et al. Intracranial compliance assessed by intracranial pressure pulse waveform.脑科学。 11, 971 (2021).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Zacchetti, L., Magnoni, S., Di Corte, F., Zanier, E. R. & Stocchetti, N. Accuracy of intracranial pressure monitoring: systematic review and meta-analysis.暴击。关心 19, 420 (2015).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Addis, A., Baggiani, M. & Citerio, G. Intracranial pressure monitoring and management in aneurysmal subarachnoid hemorrhage.Neurocrit.关心 https://doi.org/10.1007/s12028-023-01752-y(2023)。
de Moraes, F. M. et al. Waveform morphology as a surrogate for ICP monitoring: a comparison between an invasive and a noninvasive method.Neurocrit.关心 37, 219–227 (2022).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Hassett, C. E. et al. Assessment of cerebral autoregulation using invasive and noninvasive methods of intracranial pressure monitoring.Neurocrit.关心 38, 591–599 (2023).
文章一个 PubMed一个 Google Scholar一个
Brasil, S. et al. Contribution of intracranial pressure to human dynamic cerebral autoregulation after acute brain injury.是。J. Physiol。调节。集成。comp。生理学。 324, R216–R226 (2023).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Brasil, S. et al. Critical closing pressure and cerebrovascular resistance responses to intracranial pressure variations in neurocritical patients.Neurocrit.关心 https://doi.org/10.1007/s12028-023-01691-8(2023)。
Bentéjac, C., CsörgÅ‘, A. & MartÃnez-Muñoz, G. A comparative analysis of gradient boosting algorithms.艺术品。Intell。修订版54, 1937–1967 (2021).
文章一个 Google Scholar一个
Frigieri, G., Robba, C., Machado, F. S., Gomes, J. A. & Brasil, S. Application of non-invasive ICP waveform analysis in acute brain injury: intracranial compliance scale.重症监护医学。经验。 11, 5 (2023).
文章一个 PubMed一个 PubMed Central一个 Google Scholar一个
Czosnyka, M., Matta, B. F., Smielewski, P., Kirkpatrick, P. J. & Pickard, J. D. Cerebral perfusion pressure in head-injured patients: a noninvasive assessment using transcranial Doppler ultrasonography.J. Neurosurg。 88, 802–808 (1998).
文章一个 CAS一个 PubMed一个 Google Scholar一个
Chan, K. H., Miller, J. D., Dearden, N. M., Andrews, P. J. & Midgley, S. The effect of changes in cerebral perfusion pressure upon middle cerebral artery blood flow velocity and jugular bulb venous oxygen saturation after severe brain injury.J. Neurosurg。 77, 55–61 (1992).
文章一个 CAS一个 PubMed一个 Google Scholar一个
道德声明
竞争利益
G.F. is brain4care’s founder. D.C. is brain4care’s research director. S.B., M.C., and X.H. are scientific advisors for brain4care. The other authors declare no competing interests.
附加信息
Publisher’s note关于已发表的地图和机构隶属关系中的管辖权主张,Springer自然仍然是中立的。
补充信息
权利和权限
开放访问本文均根据创意共享归因4.0国际许可,允许以任何媒介或格式使用,共享,适应,分发和复制,只要您适当归功于原始作者和来源链接到Creative Commons许可证,并指示是否进行了更改。The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material.If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.要查看此许可证的副本,请访问http://creativecommons.org/licenses/4.0/。重印和权限
引用本文

Frigieri, G., Brasil, S., Cardim, D.
等。Machine learning approach for noninvasive intracranial pressure estimation using pulsatile cranial expansion waveforms.NPJ数字。医学 8, 57 (2025). https://doi.org/10.1038/s41746-025-01463-y
已收到:
公认:
出版:
doi:https://doi.org/10.1038/s41746-025-01463-y